
|
|
||
05/19/10 |
|
|
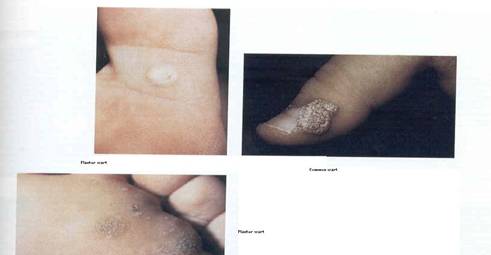
This site seeks to give users the very basic knowledge about HPV - the human papilloma virus, that is responsible for many warts and most famously, cervical cancer.HPV – Human Papilloma Virus Classification The Human Papilloma virus (HPV) is a nonenveloped double stranded, super coiled DNA virus that belong to the Papillomavirus genus and the family Papillomaviridae. It is a ubiquitous virus that is associated with many different warts such as hand, planter and anogenital warts and some genital tract malignancies such as cervical and penile cancers. HPV can also cause some epithelial tumors of the skin such as squamous cell carcinoma, or aerodigestive tract disorders and epidermodysplasia verruciformis lesions that are malignant. HPV is also found in 20-25% of head and neck cancers among men. It consists of more than 100 genotypes, based on DNA codes for their capsid proteins and is classified into super groups. Super group A consist of genital/mucosal papillomaviruses, super group B consist of cutaneous/epidermodysplasia verruciformis lesions and super group E represents cutaneous lesions such as hand and planter warts, and some animal papillomaviruses. Papillomaviruses are species specific, therefore, HPV can only infect human. Cross species infection has not been known to occur. HPV is classified as either low risk HPV, for example warts caused by HPV 6 and 11, or high risk types that could cause malignancies such as HPV 16 and 18. HPV Replication Cycle The knowledge of HPV replication cycle is not completely clear. After entering a basal cell it remains there as a non-expressed or in a latent state until the HPV episome initiates its replication based on the stage of differentiation of keratinocytes in the squamous epithelium. It generates approximately 20-50 copies of viral particles per infected cells. The viral DNA first unwinds from the super coiled state and histones are displaced and use cellular DNA polymerase and other cellular products to replicate. After replication it is packaged and may be passively released from the cell. The replication of HPV infection of cells in the lab has not been very successful and is therefore studied via molecular biology techniques. Information about the initial replication steps such as how the virus attaches to epithelial cells, endocytosis, uncoating of viral genome and transport to the nucleus, transcription and translation, is very limited. It is however know that production of viral particles occur in differentiated keratinocytes. HPV infection occurs only in actively dividing cells in the mitotic phase of the cell cycle (where nuclear membrane is broken down). The genome of HPV consists of 8 open reading frames (ORF) that are assigned early genes and late genes labels. The early genes encode non-structural proteins and the late genes code for capsid proteins. Epidemiology There are approximately 400,000 to 500,000 diagnosed cases per year of cervical carcinoma, with 80% of these found in developing countries. In the United States there is an estimated 6.2 million new HPV infections each year with 4000 deaths from cervical carcinoma occurring. Half of these deaths are in women who have never been screened and 10% are in women who have not been screened within the past five years. Ninety percent of infections clear within two years and 10%-13% of infections progress to high grade lesions and eventually cervical cancer. A survey of HPV prevalence in cervical carcinomas in the U.S. found HPV 16 to be the most prevalent strain (50%) followed by HPV 18 (14%), HPV 45 (8%) and HPV 31 (5%). However geographic variations exist with these statistics, with HPV 18 being more prevalent than HPV 16, in places such as Indonesia. While HPV infections are endemic, they do not display epidemic proportions. Factors such as transmission, incubation period, latency and spontaneous resolution tend to contribute to the lack of epidemic HPV infections. Using highly sensitive assays, cervical HPV prevalence in women with normal cytology is between 5 to 45%, with a peak for young adults in their thirties. About 74% of HPV infections occur in 15-24 year olds. About 20-30% of infected women endure multiple HPV type infections. Repeated test of individuals with HPV indicates that not all patients will be positive for every consecutive test, and may be due to latency or spontaneous resolution. Men that were asymptomatic were found to carry the virus in their genitalia and some was detected in urine and semen. There has been a direct association between the number of sexual partners and cervical cancers. Formal screening for anal precancer and cancer do not exist. Penile cancers occur in approximately 1/100,000 men in the United States, with HPV-16 implication in 80% of cases. Oral and oropharyngeal cancers are highly fatal and affect about 30,000 persons per year, with HPV implication in a large number of cases and about 87% of these being associated with HPV-16. Cutaneous warts (common planter warts or flat warts) are most prevalent among school age children. Heated swimming pools and communal bath areas tend to promote the acquisition of planter warts. There is also a strong association between immunodeficiency and the association acquisition of cutaneous warts. Patients with lymphomas experience a tenfold increase in cutaneous wart infections and patients with HIV experience 4-12 fold increase in cutaneous wart infections. Organ transplant patients are also prone to HPV cutaneous wart infections in areas of their body that is exposed to sunlight. Another demographic that experiences persistent hand warts are people working in the meat industry. Genital HPV incidence is approximately 5.5 million new cases annually in the United States (the most common STD). Estimates propose that approximately 20 million Americans are actively infected, with 500,000 -1 million people experiencing symptomatic genital warts due to HPV 6 and HPV 11 infections. During their lifetime, almost three quarters of the population may have been infected with genital HPV. Recurrent Respiratory Papillomatosis (RRP) affects 7/100,000 children whose mothers have genital warts and experience vertical transmission during the birth of the baby. Pathogenesis Oncogenic types of HPV are HPV 16, 18, 31, and 41. Other types of HPV induce warts. The incubation period of HPV infection has not been fully deciphered. In experimental inoculation, the full development of cutaneous wart lesions occurred within 3-4 months, while some occurred six weeks to two years later. Studies of natural history exposure to infected sexual partners produced a range of incubation periods. Generally, HPV infects keratinized skin cells, and has also shown to successfully infect the mouth, upper airways, vagina, cervix and anal canal. Other tissues such as the conjunctiva, lacrimal sac, nasal passage, esophagus and bladder have also been positive for infection is some people. Malignancies occur after transformation of latently infected cells and may take several years to decades to develop. During latency, viral particles are not produced and no histopathological changes are detected. Factors that contribute to latency are unknown. Transformation of an infected cell to malignant cell begins with the integration of HPV genome into the host cell gene. This occurs in most cervical carcinomas, and is rare in benign an pre-malignant lesions. Integration generally disrupts the viral and cellular regulatory controls. Protein products are produced which interferes with tumor suppression gene factors of the cell. Transmission Cutaneous warts are transmitted via personal contact. If the skin is traumatized, the risk of transmission is greatly increased. Planter warts are indirectly transmitted via fomites in places such as communal baths and pools. Anogenital warts and other HPV infections are strongly associated with sexual transmission. However, only some HPV infections in this area will result in lesions. Infections with HPV in the anogenital regions are related to the onset of sexual activity and the risk increases with an increasing number of sexual partners. It was also found that sexual partners also share the same HPV infections or diseases. Respiratory papillomatosis (altered cry in infants or adult hoarseness) which is more sever in children than in adults, is due to respiratory distress because of the growth of HPV lesions within the respiratory pathway. Young children can acquire this via passage through an infected birth canal. In adults, onset is due to oral sex and infections can possibly undergo malignant transformation. Nosocomial infections may be due to viruses being in fumes of laser therapy. It is resistant to heat and therefore cause persistent infections. Laser surgeons seem particularly prone to hand and nasopharyngeal warts. Clinical Manifestation Warts There are three major types of cutaneous warts, namely, deep planter warts, common warts and flat warts. Deep planter warts are usually isolated and found on the weight bearing surfaces of the foot. They may appear as a corn or callus because the lesion is covered by keratotic rings. Common warts form numerous lesions that have a course surface. They are generally located on the dorsal part of the hand, between fingers and nail bed (and possibly grow under the nail bed which can result in nail loss). Another type of common wart called mosaic wart is found on the foot, knuckles, and around toenails. These warts are painless. There is an also filiform wart that occurs on the face. Malignant transformation of warts may be due to the presence of oncogenic HPV types in the lesions. In a 1-5 year follow-up of children infected with cutaneous warts, spontaneous resolution can occur in 1-2 months. Plane and flat warts found on the face, most commonly, may regress within 2-7 weeks. However, patients that are immunocompromise, lesions appear as warty keratosis, where malignant and benign lesions have been shown to contain HPV.
Images obtained from Clinical Virology, Richman, D. et.al., 2nd edition Epidermodysplasia Verruciformis (EV) This is the appearance of flat-wart like lesions on the face, torso and extremities, during the initial ten years of infection. It can contain more than twenty different types of HPV and HPV-3 is closely related to these warts. These patients also have planter and common warts more often. In about 50% of patients with EV experiences malignant and premalignant transformations to papillomas sebhorric keratosis, and squamous cell carcinoma. Malignant lesions are locally invasive. These lesions are associated with HPV 5, 8, and 47. HPV can also cause papillomas and malignant tumors of the conjunctiva and HPV 5 has been shown to be associated with psoriasis skin lesions.
Images obtained from Clinical Virology, Richman, D. et.al., 2nd edition EV with plaque like manifestation caused by HPV, and multiple primary squamous cell carcinoma on the forehead of a man with EV caused by HPV 8 Recurrent Respiratory Papillomatosis This infection is marked with hoarseness among adults and an altered cry in infants. There is some degree of respiratory distress that is caused by smooth or fungating lesions that occur where ciliated and squamous epithelia juxtapose. There could be extra laryngeal spread in children (31%) and adults (16%). These lesions can grow towards the lungs and may require surgical removal or they can result in asphyxiation. These lesions comprise HPV 6 and HPV 11. There is a small percentage of malignant transformation in this infection (less than 10%). In general, infection of the oral mucosa with HPV produces common warts, condylomas and squamous cell papillomas, all distinguished by their histology and HPV type they contain. Anogenital HPV Diseases Anogenital HPV infections can be better diagnosed depending on information provided by patients. This includes a sexual history of the patient (time of first intercourse, number of sexual partners, who their past and current partners are, sexual practice and which, if any, barrier contraception was used. Symptoms of infection, symptoms during urination and defecation, and sexual intercourse, history of other STD and treatment received, and a history of anogenital warts, and malignancies in their partners. Testing can also provide a more definitive diagnosis. Condylomata acuminata (CA) are anogenital warts that are hairless and may be formed singly or coalesce to form a plaque. Men usually experience lesions on the penile shaft and preputial cavity. Urethral warts occur in 1-25% of patients and usually do not go beyond the distal first 3cm, therefore rarely involve the urethra and bladder. The scrotum, perineum, groin and pubic areas rarely experience this infection. Lesions in women are found mostly spreading toward the labia minora and majora and clitoris. CA is marked with itching, burning, pain and tenderness. Most patients are asymptomatic (approximately 75%) and 10-20% may experience spontaneous resolution. However, pregnancy and immunosuppression can cause the warts to increase in size, blocking the birth canal. Warts on the genitals undergo involution and then spontaneously disappear.
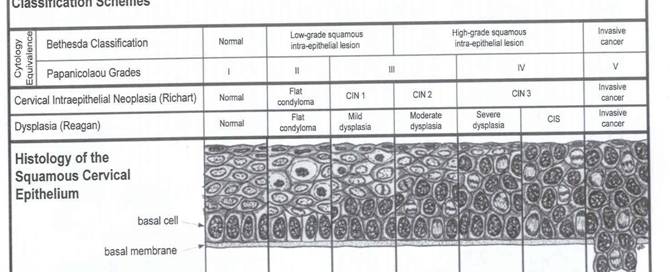
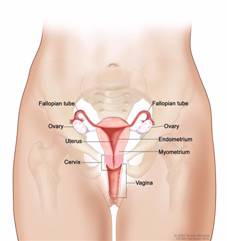
Images obtained from Clinical Virology, Richman, D. et.al., 2nd edition (female with CA – HPV 6 association and male with CA on penis) Among women with genital warts, cervical warts occur in less than 10% of infected women. Intraepithelial neoplasias can display the multicentric quality of HPV infection by the existence of lesions in different anatomic locations such as the penile intraepithelial neoplasia (PIN), vulvas intraepithelial neoplasia (VIN), vaginal intraepithelial neoplasia (VAIN) and anal intraepithelial neoplasia (AIN). Intraepithelial neoplasias, verrucous carcinomas and squamous cell carcinomas have all been associated with HPV DNA, and in particular HPV 16 DNA. Cervical Carcinoma Preinvasive and invasive cervical cancer sometimes develops after infection with high risk genotyped (HPV-16, HPV-18, HPV-31 and HPV-45). HPV-16 antibodies are found in cervical cancers and its prevalence increases as the cancer develops. Cervical cancer occurs in the cervix (lower part of the uterus) and is symptomless in the early stages (called dysplasia). As the cancer develops, there may be symptoms such as vaginal discharge and unusual bleeding. In advanced stages of cervical cancer, symptoms include heavy bleeding, weight loss, pain, fatigue and loss of appetite. It is a slow developing cancer (years) that begins in the squamous cells on the surface of the cervix, and symptoms only become apparent when the cancer is in the advanced stages of development.
Prevention The prevention of HPV spread can be maximized by the proper sterilization of surgical instruments used on infected patients, and the proper disposal of materials. Contaminated surfaces can be sterilized with household bleach (1:10 dilution). For those people who have warts, the proper dressing over the warts can be useful in preventing spread of HPV. The use of condoms for all sexual activities is highly advisable, although its efficacy is still unclear. During electro and laser surgery, a smoke evacuation system should be used so that the virus is not spread when fume is disseminated. The avoidance of UV light exposure in immunocompromise patients with EV is highly recommended, so as to prevent risk of malignant transformation. Currently there are two HPV vaccines available to prevent infection with some HPV viruses. These are Cervarix (by GlaxoSmithKline) and Gardasil (by Merck). Gardasil protects against HPV 6, 11, 16, and 18. Cervarix protects against HPV 16 and 18 only. Gardasil has been shown to prevent cancers of the vagina and vulva along with cervical cancers (all caused by HPV 16 and 18). Cervarix has not been implicated as of yet in prevention of vulva and vaginal cancers. There is also the possibility that Gardasil and Cervarix may prevent head, neck, penis, and anal cancers due to HPV 16 and 18 infection, and recurrent respiratory papillomatosis caused by HPV 6 and 11. About 70% of cervical cancers are caused by HPV 16 and 18. Both of these vaccines also prevent precancers in women. They were developed using small parts of the HPV that are noninfectious (called virus like particles or VLP. HPV 6 and 11 are the causative agents of most genital warts in women and men. Gardasil and Cervarix are vaccine adjuvant that utilized a very small amount of inactivated virus in conjunction with aluminum gel or aluminum salt, to produce a magnified immune response. Gardasil ( approved in June 2006) and Cervarix have both been licensed by the FDA, and are safe and effective for girls ages 9-26 years and males 9-26 years old (approved by the FDA in October 2009). It is administered in three doses beginning when girls are 11-12 years old. The second dose of HPV vaccine has to be administered two months after the first dose and the third dose is administered six months after the first dose. The side effects of these vaccines include pain at the location where the vaccine was given, fever, headache and nausea. There has been no major side effect noted to date. The benefit of HPV vaccines may be extended to people who were sexually active before getting all three doses, if there is a chance that they did not get infected as of yet. If someone is however infected with HPV, the vaccine will not be effective in treating warts or cancers. The best recommendation for maximum vaccine efficacy is to get all three doses before sexual activity begins. HPV vaccine has been added to the vaccine schedule for girls but NOT boys, because some studies have determined that vaccination of as many girls or women as possible is the most effective way to prevent diseases due to HPV infection. Gardasil was approved for men and boys to prevent genital warts caused by HPV 6 and 11. Treatment Patients infected with HPV are currently treated with physical or chemical agents. Two of the most common chemical treatments are Podofilox (Condylox) and Imiquimod (Aldara). There is 45-90% clearance of infection with the use of Podofilox because it destroys the wart tissue, but 30-60% recurs after use of this treatment. Podofilox has to be used for four weeks. Imiquimod enhances the immune response against the virus and there is 70-85% clearance of the infection, but 5-20% infections returns. There has also been vaccine development that effectively prevents infection among uninfected individuals. If one treatment is not effective after 3-6 treatments, then other treatments are tried. Physical methods of treatment include curettage of cutaneous warts which can be painful and leaves scarring. Cold blade excision of anogenital warts is very effective and was also used in biopsy of CIN, which is now treated with electrosurgical techniques. Micro receptors (biopsy forceps) are also used for the resection of laryngeal papillomas. Electro surgery uses electric current to ablate infected tissues and this treatment varies (in terms of the number of electrodes used, amperage, voltage, and wave form) according to the tissue being treated. It can be painful and leaves scarring (therefore it is used under local anesthesia). Cryotherapy (treatment by cold) can be done using any one of three treatments: - carbonic ice (boiling temperature -78.5oC), nitrous oxide (-89.5oC), and liquid nitrogen (-196oC). When applied using a cryogenic pencil, there was transmission of the virus, thus liquid nitrogen spray proved to be safest. Cryotherapy produces an ice ball around the lesion and is accompanied by a little bit of pain that subsides after thawing, and there is minimal scarring. Laser therapy used to treat HPV lesion consist of high energy monochromatic, collimated light delivered via lasers such as the CO2 laser. Light produced by lasers is absorbed by water within the cell which results in vaporization of the liquid. A local anesthesia has to be used so as to alleviate any pain during treatment. Photodynamic lasers work by applying photosensitizing agents to the HPV lesions (such as cutaneous warts, genital HPV diseases and recurrent respiratory papillomatosis) which is activated to selectively destroy that tissue when exposed to light of specific wavelength. During the precancerous phase of dysplasia, treatment can be 100% effective and is normally identified in Pap smear. The cases of advanced cancer occur in women who have not been screened or have missed at least five years of screening. Early stages of precancers can be treated with LEEP (Loop Electrosurgical Excision Procedure), where abnormal tissue is removed with the use of electricity, Cryotherapy and laser surgery. Patients who have had LEEP procedures and still get cervical cancer generally are advised to have a hysterectomy. In more advanced cases, most of the pelvic organs are removed (such as the bladder and rectum). Radiation and chemotherapy are also used to treat the cancer either before or after surgery.
|
This site was last updated 05/19/10




 Picture
obtained from
Picture
obtained from